
Question: Is a Semaglutide like Wegovy safe for weight loss?
Answer: Semaglutide is generally safe for weight loss, but it can have side effects and may not be suitable for everyone. You should only consider using it under a doctor’s care.
Semaglutide belongs to a class of medication known as GLP-1 RAs that mimics hormones that are released in the gut in response to eating. It has been used for years to in treating Type 2 diabetes because it prompts the body to produce more insulin and reduces blood sugar levels.
In 2021, the FDA approved Semaglutide for weight management. It has been shown to be safe and effective for two years. It has also been shown to lower the risk of serious cardiovascular problems in some people with heart disease.
But there are side effects. These include: nausea, vomiting, and diarrhea, especially in the first few months. Other less common side effects include: allergic reactions, change in vision, dehydration, gallbladder problems, pancreatitis and others.
People with a history of pancreatitis should discuss the safety of semaglutide with their doctor and people with a history of medullary thyroid carcinoma should not use semaglutide
You should talk to Dr. Weisz to learn more about semaglutide and the best chronic weight management option for you.
Got a Question? Send it to drw@weiszconciergemedical.com and, if it is of general interest, Dr. Weisz will provide an answer in an upcoming issue of the Concierge Connection.
===========================================================================

New Osteoporosis Screening Guidelines for Older Women
A government task force has released updated recommendations for osteoporosis screening to help prevent fractures. These recommendations focus on women aged 65 and older. The key points of the new recommendation are:
- All women aged 65 and older should be screened for osteoporosis.
- Postmenopausal women under 65 should also be screened if they have at least one risk factor (e.g., low body weight, family history of hip fractures, smoking, heavy alcohol use).
Screening Methods:
The task force recommends using central dual-energy x-ray called DXA to measure bone mineral density (BMD) at the hip or lumbar spine.
Risk assessment tools like FRAX (Fracture Risk Assessment Tool), which predicts the 10-year fracture risk based on clinical factors, are also used to identify women who should be screened.
Changes from 2018 Guidelines:
The current guidelines shift from using a formal clinical risk assessment tool for all women to focusing more specifically on screening those at increased fracture risk.
The task force no longer uses BMD testing alone to assess risk in younger women under 65. Instead, clinical risk assessments are first used to determine the need for screening.
What about men?
There is insufficient evidence to recommend routine osteoporosis screening in men, and doctors should use their judgment about fracture risks when considering screening in male patients.
What are fracture risks?
Studies reviewed by the task force found that osteoporosis screening was linked to a reduction in hip and major osteoporotic fractures, with five fewer hip fractures and six fewer major fractures per 1,000 participants screened.
Treatment Options:
If screening identifies a need for treatment, drugs such as bisphosphonates are recommended. The task force also highlighted that fixed risk thresholds may not be fully accurate for diverse racial and ethnic groups or for patients with diabetes.
In summary, the updated guidelines recommend osteoporosis screening for women at risk, with a focus on using clinical risk assessments and DXA scans for more accurate fracture prediction. However, there are ongoing challenges with risk assessment tools and their applicability, particularly in younger women and men.
===========================================================================
Source: Monaco, Kristen. US Preventive Services Task Force “Screening for osteoporosis to prevent fractures: US Preventive Services Task Force recommendation statement” JAMA 2025.
===========================================================================

Beyond BMI: Alternative Measures of Body Fat
Medical experts from around the world are calling for a significant overhaul in how obesity is diagnosed, moving beyond the traditional reliance on Body Mass Index (BMI). A global commission endorsed by over 75 medical organizations, argues that BMI alone is insufficient to accurately diagnose obesity, as it can both overestimate and underestimate body fat. Instead, they propose using additional measures of body fat, such as waist circumference or direct fat measurements, alongside individual health signs and symptoms.
The commission introduced two categories of obesity: clinical obesity and preclinical obesity. Clinical obesity is characterized as a chronic illness caused by excess body fat, leading to organ dysfunction and limitations in daily activities. It requires a diagnosis that includes not only excess body fat but also clear signs of organ dysfunction or reduced mobility.
Preclinical obesity, on the other hand, involves excess body fat without significant organ dysfunction but is associated with a higher risk of developing diseases like cardiovascular conditions and type 2 diabetes.
The proposal aims to reframe obesity as a disease, allowing for more personalized care. For individuals with clinical obesity, timely interventions such as medications or surgery may be necessary. Those with preclinical obesity might benefit from preventive measures like diet and exercise. The commission also suggests that additional diagnostic tools—such as waist-to-hip ratio or advanced imaging techniques like DEXA scans—should be used, particularly when BMI is less informative.
This new approach is seen as an attempt to improve diagnostic accuracy, provide more tailored treatments, and better allocate healthcare resources for obesity management.
===========================================================================
Source: Rubino F, et al “Definition and diagnostic criteria of clinical obesity” The Lancet Diabetes & Endocrinology. 2025;
===========================================================================

New Finger-prick Test Used to Diagnose Alzheimer’s
A recent study presented at the 17th Clinical Trials on Alzheimer’s Disease (CTAD) conference explored the potential of using a simple finger-prick blood test to identify a key biomarker for Alzheimer’s disease (AD). This test could offer an easier, more accessible alternative to traditional venous blood sampling, which requires specialized infrastructure, immediate processing, and cold storage.
In the pilot study, researchers compared p-tau217 levels in venous blood and capillary blood samples (from a finger prick) in 206 adults, with or without cognitive impairment. The findings showed a strong correlation between the two sample types, suggesting that finger-prick samples could be used for AD diagnosis. Notably, the finger-prick samples, once dried on a plasma spot card, were stable for up to two weeks at room temperature and could distinguish between amyloid-positive and amyloid-negative individuals, as well as different stages of cognitive decline.
The research, part of the DROP-AD project, indicates that finger-prick blood collection is not only feasible but could also be a cost-effective, widely accessible tool for clinical settings and trials, especially in remote areas. While the results are promising, the technology still requires broader validation before it can be used in clinical practice. The Alzheimer’s Association noted that while the idea is exciting, further research and systematic review are necessary before implementation.
In conclusion, a simple finger-prick test for Alzheimer’s biomarkers could significantly improve early diagnosis and treatment, although more studies are needed to confirm its reliability and clinical applicability.
======================================================================
Source: Brooks, Began. Medscape Medical News. Finger-Prick Test for Alzheimer’s Disease? November 01, 2024
===========================================================================
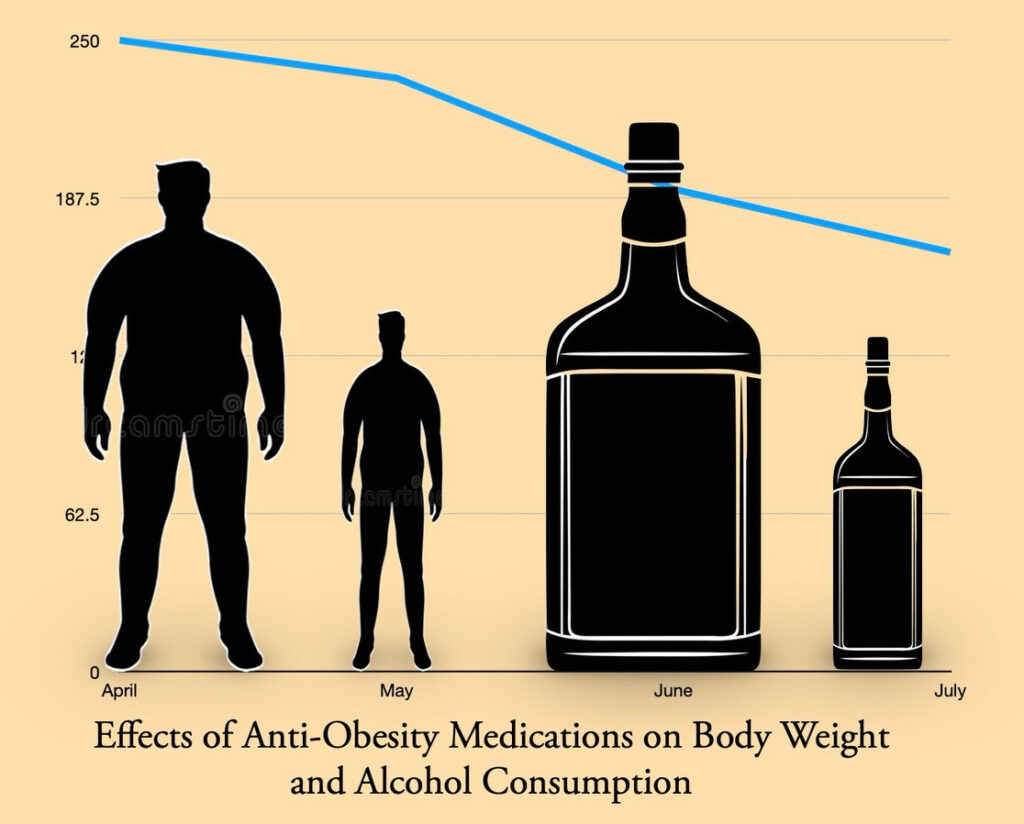
Anti-Obesity Meds Lower Alcohol Consumption
A recent study presented by the Obesity Society revealed that anti-obesity medications , including GLP-1s like Ozempic, are associated with decreased alcohol consumption. Researchers surveyed over 14,000 participants from WeightWatchers’ telehealth weight management program. Key findings of the study include:
Reduction in Alcohol Use: About 45% of participants who consumed alcohol reported drinking less after starting anti-obesity meds (AOMs), with reductions increasing among those who initially drank more. Only 2% reported increased alcohol consumption.
Similar Results Across AOM Types:
Various AOM classes, including metformin and bupropion showed similar reductions in alcohol consumption.
Potential Mechanisms:
The decrease appears to stem from both biological effects (reduced cravings and negative physical responses to alcohol) and intentional health-focused behavior by patients aiming to improve overall wellness.
Demographic Trends:
Men, as well as individuals with higher obesity classes, were more likely to experience decreases drinking.
The findings suggest AOMs may influence alcohol consumption via shared brain reward pathways and intentional lifestyle changes. Further research is needed to compare AOMs with non-pharmacological weight management approaches for reducing alcohol use.
===========================================================================
Source: Tucker, Miriam, E. Medscape Medical News. November 23, 2024.
===========================================================================

Does Light-Intensity Walking Benefit Your Blood?
A recent study produced these findings about the connection between high-intensity walking and blood glucose levels:
- Light-intensity walking reduces glucose levels and blood pressure in young adults with obesity.
- Walking patterns, whether continuous (30 minutes) or intermittent (3 minutes every 30 minutes), can also lower insulin concentrations.
- Triglyceride levels and blood pressure did not show significant changes across different walking conditions
Methodology:
A randomized crossover trial with 16 young adults (ages 18–34, BMI ≥ 25) was conducted in Bangkok, Thailand.
Participants engaged in four experimental conditions over separate 7-hour periods:
- Uninterrupted sitting
- 30 minutes of light-intensity walking
- 3-minute bouts of light-intensity walking every 30 minutes
- A combination of continuous and intermittent walking.
Glucose, insulin, triglycerides, and blood pressure were measured and compared.
Conclusions:
- Light-intensity walking, regardless of pattern, improves glycemic control and reduces blood pressure.
- Timing and walking patterns may be important for reducing insulin levels.
Limitations:
- Small sample size (16 participants) limits generalizability.
- Short study duration (7 hours) and controlled setting may not reflect real-world conditions.
- Lack of objective physical activity measurement and variability in dietary control are additional limitations.
Implications:
This study suggests that light-intensity walking is a practical and effective intervention to manage blood glucose and blood pressure in young adults with obesity. Future studies are needed to explore long-term effects and real-world applicability.
===========================================================================
Source: Bhattacharya, Shrabasti. Medscape Medical News. November 19, 2024.
===========================================================================
Laughter is the Best Medicine


===========================================================================
Butternut Squash and Kale Torte


This is how vegetarian fare should taste
Layered like lasagna with flavorful vegetables and nutty cheese. If the torte feels too fancy, prepare it casserole-style in a baking dish and serve by scooping out portions.
Ingredients:
- 1 Tbsp. olive oil
- 1/2 small butternut squash (about 1 lb)
- 1 medium Red Onion
- 1 small bunch kale
- Kosher salt and pepper
- 1 medium Yukon gold potato (about 6 oz)
- 6 oz. thinly sliced provolone cheese (from the deli counter)
- 1 plum tomato
- 1/4 cup grated Parmesan (1 oz)
- Crusty bread, for serving
Preparation:
STEP 1
- Heat oven to 425°F. Oil a 9-in. springform pan. Arrange half the butternut squash in the bottom of the pan, in concentric circles. Top with half the onion, separating the rings. Top with half the kale, drizzle with half the oil and season with 1/4 tsp salt. Top with the potatoes and half the provolone cheese.
STEP 2
- Top with remaining kale, drizzle with the remaining oil and season with 1/4 tsp each salt and pepper. Top with the remaining onion, tomatoes and provolone. Arrange the remaining squash on top and sprinkle with the Parmesan.
STEP 3
- Cover with foil, place on baking sheet and bake for 20 minutes. Remove foil and bake until the vegetables are tender and the top is beginning to brown, 8 to 10 minutes more.
Tips and Tricks: Remove kale stems quickly with this easy method: Fold the front of the leaf in half lengthwise, exposing the stem in the back. Using a sharp knife, cut away the stem..
Source: WOMAN’S DAY KITCHEN Published: NOV 6, 2014.